


Dr. Japanacharya
Sorry Boomers. You gotta go. You gotta get off this rock as your medical bills are a problem for the Scorpions. More on Trump's pick for NIH, Dr. Jay Bhattacharya
National Bureau of Economic Research
https://www.nber.org/bah/2017no2/featured-researcher-jay-bhattacharya

Jay Bhattacharya is a professor at the Stanford University School of Medicine, as well as a professor (by courtesy) in the department of economics and the department of health research and policy at Stanford. He is a research associate in the NBER's Health Care and Health Economics programs.
Bhattacharya's research aims to understand the constraints that vulnerable populations face in making decisions that affect their health status, and in particular how government policies designed to benefit these populations actually affect the lives of people in such groups. More recently, his research has focused on the links between biomedical science and health. Some recent projects explore the use of "nudges" in exercise commitment contracts, the health consequences of population aging in Japan, the cost of treating highly complex patients in Medicare, and the incentives faced by biomedical scientists to try out new ideas in research.
Bhattacharya is a senior fellow at the Stanford Institute for Economic Policy Research and the Stanford Freeman Spogli Institute, and has been a research fellow at the Hoover Institution. Prior to joining the Stanford faculty, he was an economist at the RAND Corporation and taught classes in the economics department at UCLA.
Bhattacharya received his Ph.D. in economics, A.M., and A.B. degrees from Stanford. He is an M.D., also earned at Stanford.
He has served on numerous scientific review and advisory committees, including the Health Services Organization and Delivery review panel at the National Institutes of Health and an Institute of Medicine panel on the regulation of work hours by resident physicians. He has provided testimony to the California State Legislature. He is an associate editor at the Journal of Human Capital and an editorial board member of the Forum for Health Economics and Policy. He previously served as associate editor of the Journal of Human Resources and the Economics Bulletin. Bhattacharya has published a textbook, Health Economics, which he is preparing to revise for a second edition.
Allow me to decode some of this.
I speak Rand.
Dr. Jay Bhattacharya is a public health economics bean counter.
That’s why he was installed as a fake dissident on lockdowns whilst pushing the shots on the problematic olds.
It’s Depopulation.
Yep. Sure as shit is.
You can call it “iatrocide” or whatever Swarthmore term for killing people in hospitals or “eldercide” or just WE NEED SOME PEOPLE DEAD RAPIDO-CIDE.
(:27 video)
“Honestly, there may be viewers who won’t take it (the Kovid Death Shot) from Anthony Fauci but might take it from Jay Bhattacharya…”
(1:26 video)
“…to protect the vulnerable older people…”
Donald Trump is 100% part of the Operation to clean up that aging demographic population and their Useless Eaters.
He is just the face of Clear Coat branding and his team is in place to make sure the agendas go through.
It’s the United States running point here.
This plan spans cross-Presidential fake paradigm lines.

You can argue all day long about Pfizer or DOD or State Department or Chyyynnaaa but this is plain as day a coordinated global operation that supersedes Steak Sales Boys and Bear Boy Heroin junkies or Demented Delaware Credit Card Company Boys or Kackling Kamalas.
(:22 video)
“We really also need to expand our global vaccination program…”
The “we” and “our” is the United States WHOLE OF GOVERNMENT.
“Vaccinations” are simply the finest way to murder people…slowly…with a modicum of plausible deniability.





"In every case, total medical spending for the elderly will increase dramatically between 2005 and 2030 because the elderly population will increase dramatically during that period"
"Modeling the Health and Medical Care Spending of the Future Elderly", Dr. Jay Bhattacharya's 2008 Rand Corporation Conclusion
Remember that whole “Death Panels” debate?
Yeah.
This may be the angle that red pills people who can’t stomach DEPOPULATION or EUGENICS or EUTHANASIA or FAKED PANDEMICS or JABS BAD…
But understand ECONOMICS.
To be clear, I write this Stack not as an advocacy site but rather as a “solve the mystery” site.
Meeebbbeeee have this case solved and it’s time to head to Wanda’s Diner for some chili now!
Note: Some bolding is mine. I picked the Cancer Section because it is illustrative of what I think is the dominant mechanism of culling the herd being deployed.
Excerpt is provided, full paper is here. RAND Corporation exploration into Modeling the Health and Medical Care Spending of the future Elderly, busted out in 2008, which points to this current timeline.
Trump’s NIH nod Dr. Jay Bhattacharya, Stanford Public Health dude, is an author.
https://www.rand.org/pubs/research_briefs/RB9324.html
Wrote the Economist Bean Counter WITH AN MD! ::wink-wink:: for the United States Military Think Tank, Rand Corporation in 2008:
Effects of Cancer Treatment on Medicare Spending
Cancer is largely a disease of old age. For example, about 60 percent of cancer patients in 2001 were age 65 or older. Because cancer treatment is expensive, changes in cancer treatment would certainly affect Medicare spending. A team of analysts used FEM to project spending on cancer care among the elderly through 2030.
To capture the uncertainty about the nature of future cancer treatment, the team estimated the future costs of treatment using five widely varying scenarios of technological change:
Cancer treatment technologies existing in 2000 remain the same until 2030.
New drugs developed between 2000 and 2004 improve treatment outcomes.
Cancer screening technologies improve significantly.
A cancer vaccine is developed.
A cure for cancer is discovered.
These scenarios, which range from very pessimistic to very optimistic, reflect the judgments from a panel of experts on cancer and the biology of aging. Some of the scenarios would keep some people alive long enough to contract other diseases. If these diseases are expensive to treat, a relatively inexpensive and effective cancer treatment could end up increasing Medicare spending. An important feature of FEM is its ability to model the outcomes of such competing mortality risks.
Figure 3 shows FEM's projection of cancer prevalence among the elderly, based on each of these scenarios. (Prevalence is the number of individuals age 65 and over reporting having cancer in a given year, divided by the total number of individuals age 65 and over in that year.)
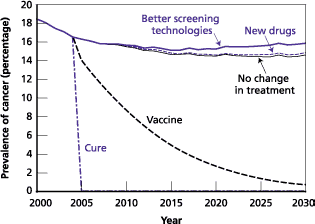
If there is no change in treatment, cancer rates decline from close to 20 percent in 2000 to about 16 percent in 2015 and then remain unchanged through 2030. The decline reflects the fact that people aging into Medicare between 2000 and 2015 were healthier than previous beneficiaries because the former group had lower smoking rates. By 2015, this replacement process reaches a steady state.
In two cases, the scenarios increase the prevalence rate. New drugs could increase the survival rate, so that at any given time there would be more people alive with cancer. Better screening technologies would increase cancer prevalence because previously undetected cancers would be found at an early stage, and early-stage cancer patients are more likely to survive.
Both a vaccine and a cure would reduce cancer prevalence. In the case of a vaccine, prevalence would essentially reach zero after the remaining cancer survivors die. In the case of a cure, cancer prevalence would drop immediately to zero.
However, none of these scenarios would significantly affect total Medicare spending. In every case, total medical spending for the elderly will increase dramatically between 2005 and 2030 because the elderly population will increase dramatically during that period. Demographics swamp the effects of even the most impressive technological developments.
As for Japan and their aging populace problem, interesting that our good buddy Garden Gnome Malone just did another INTERNATIONAL CRISIS SUMMIT in Tokyo.
related:


Oh look at this movie they just made for the Japanese audiences!
What a fucking world.
What a timeline.
The Scorpions are busy now.


The shots were very clearly not "pretty safe" as Dr. Jay Bhattacharya said at Hoover Institute in October, 2021.
IIRC, the UK charts were showing that even with the bullshit two week window of being categorized "unvaccinated" after one shot and then two, the elderly were dropping like flies after getting injected. (TLAV was covering this very well, before I ever emerged like bat to pangolin fake virus onto Substack.)
This is before we get to the hospital death protocols of Midazolam/Vents or Remdesivir/Vents and the separating patients from their families to be culled.
Peter Navarro of warroom fame had the same messaging as battacharya, very odd to watch someone explain how dangerous the vaccine might be and then insist elderly take it. Almost like they want them dead.